
Abstract
Introduction
Sexual and reproductive health and rights (SRHR) policies use gender as the foremost social determinant to explain vulnerability in relation to SRHR among young people. Therefore, our aim was to explore intersecting vulnerable positions within the three SRHR-related outcome areas: unsafe sex, sex against one’s will, and transactional sex, among young people aged 16–29.
Methods
The data set is from a randomised, cross-sectional, and population-based SRHR survey conducted in Sweden in 2015, and the 7755 respondents imply a response rate (26%) in line with the power estimations. How gender intersects with five other social positions, i.e. social determinants (sexual identity, transgender experience, perceived economy, being foreign-born, and social welfare recipiency), was explored through a stepwise descriptive intersecting vulnerability analysis exemplified through three outcome variables: unsafe sex, sex against one’s will, and transactional sex.
Results
Gender intersects with other social determinants and creates vulnerable positions in SRHR-related outcomes. The most vulnerable positions within each of the three outcome variables were the following: (1) for unsafe sex: being a man and homosexual; (2) for sex against one’s will: being a woman and bisexual; and (3) for transactional sex: being a man and having transgender experience.
Conclusions
Despite limitations, the descriptive intersecting vulnerability analysis indicates how gender intersects with other social determinants and generates multiple vulnerable positions in relation to SRHR.
Policy Implications
The results can be of interest in future studies on vulnerability and inform policies that intend to fulfil the intention of leaving no one behind, as stated in the Agenda 2030.
Similar content being viewed by others


Introduction
In 2018, the Guttmacher-Lancet Commission acknowledged that sexual and reproductive health and rights (SRHR) constitute a key area for health improvement (Starrs et al., 2018). The commission defined SRHR as a “… state of physical, emotional, mental, and social well-being in relation to all aspects of sexuality and reproduction, not merely the absence of disease, dysfunction, or infirmity”, and stressed that SRHR is intertwined with broader social, economic, cultural, and health care contexts. Information and services should be accessible and affordable to all who need them, regardless of their age, marital status, socioeconomic status, race or ethnicity, sexual orientation, or gender identity. Drawing on this, the commission noted that a broader view of social determinants must be taken into consideration for SRHR. It also identified young people to be a key population for SRHR interventions (Starrs et al., 2018). However, existing United Nation (UN) policies in the field of SRHR tend to focus almost exclusively on gender as the most important determinant for SRHR, and by extension also for analysing population-based surveys and the prioritisation of interventions. In this paper, we problematise the exclusivity of gender as the solitary driving determinant for the investigation of vulnerability in relation to SRHR, and our hypothesis is that intersectionality may be a useful tool to develop vulnerability analysis.
From Global to National Perspectives
The founding global policy documents on SRHR intend to guide nations who in turn develop their national strategies, and thus population-based surveys, which stems from various UN bodies. The starting point were the International Conferences on Population and Development (ICPD), and the agreements reached in Cairo in 1994 and Beijing in 1995. In these policy documents, gender mainstreaming was identified as the guiding principle for vulnerability analysis and interventions in order to promote SRHR (UN, 1995). This has led to progress in the acknowledgement of human rights and in health promotion for girls and women, and to the fact that global policy has become well informed about gender mainstreaming, i.e. gender-based analysis (Ritchie, 2012). Moreover, the General Comments to the Convention of the Rights of the Child clarify that gender discrimination affects a wide range of health outcomes (UN, 2013). For this reason, all national policies and programmes need to include a recognition of gender equality in relation to sexual and reproductive health. The WHO action plan on SRH and human rights states that all people regardless of gender identity, age, sexual identity, socioeconomic conditions, cultural background, or legal status should be able to achieve the highest attainable sexual and reproductive health and well-being (WHO, 2016). The vision addresses multiple factors for inclusion in vulnerability analyses, suggesting the need for a complex approach. However, in its discussion of verifiable goals and indicators, the complexity of the perspective outlined in the policy document disappears, as goals, activities, and indicators are mainly based on gender.
The most recent global policy from the UN, Agenda 2030, has an inclusive vision and urges all nations to “leave no one behind”, and to “improve the lives and prospects of everyone, everywhere” (UN, 2015). However, the agenda mainly focuses on gender-based analysis in accordance with the respective agreements from the ICPD conferences in Cairo and Beijing. This leaves stakeholders with a vision of gender equality and health equity in the field of SRHR that was stated more than 20 years ago, and risks leaving vulnerable groups behind. To conclude, the UN bodies’ SRHR policies appear to be exclusively focused on gender and fail to discuss how gender intersects with other social determinants.
Learning from research in the field of HIV/AIDS, we know that gender is not an exclusive driving factor in the HIV pandemic. For example, men who have sex with men, transgender people, and sexual minorities all constitute key populations in relation to policy and practice (Andersson, 2019; Persson, 2018; Persson et al., 2016; Wolitski & Fenton, 2011). This underlines the need for an intersectional perspective on social determinants in both research and policies that informs SRHR practice. In the Swedish context, previous knowledge shows that among young people, vulnerable groups with more sexual and reproductive ill health are as follows: non-binary young people (The Public Health Agency of Sweden, 2017); young people with alcohol or drug misuse (Hammarstrom et al., 2015); young people in secure state care (Schindele & Lindroth, 2020); and young men who have sex with men (Johansson et al., 2018). Sweden got its first national policy on SRHR in 2020, and it aspires to consider the multiple layers of vulnerability that needs to be addressed (The Public Health Agency of Sweden, 2020).
Theoretical Perspectives
The social determinants of health are key elements in the theory and methods that explore how social conditions affect health equity. It sheds light on how a society can address social inequalities that can be adjusted by reasonable means and improve health outcomes in vulnerable groups (Marmot, 2005; Viner et al., 2012). The most common social conditions that have been explored in relation to SRHR are gender, education, income, and class (Marmot & Wilkinson, 2005). Research on the social determinants of health is mainly conducted by means of social stratification, i.e. categorising people into analytical groups based on common social characteristics such as gender, education, and income. This is a widely used means of exploring social conditions in different subgroups, especially in national samples (Berkman et al., 2014). However, our hypothesis is that, in order to be SRHR relevant, these analytical categories also need to be informed by intersectionality and include transgender and non-binary people and sexual minorities.
Intersectionality highlights how gender-based inequality is also intertwined with other social determinants and power structures (Bowleg, 2013; Collins, 1998; Crenshaw, 1991; Gahagan & Bryson, 2021). For example, health may be affected differently if you are male only, or if you are male and gay, or male and gay and a migrant (Bowleg, 2008). Intersectionality emphasises that health is shaped through the social power relations that operate in the context of human life, and it takes a clear stand on the importance of discussing gender not in isolation but also in relation to for example ethnicity/race and sexual identity (Bowleg, 2008, 2012; Bredström, 2008; Kapilashrami, 2020). Moreover, intersectionality can reveal hidden social groups, and in doing so provide insights into the way that invisible and hidden social positions make us vulnerable to sexual ill health (Bowleg, 2013).
Previous Research
Quantitative research informed by intersectionality has been found to give more precise information on the existence of health inequalities in general health (Wemrell et al., 2021). Yet, intersectional analysis is relatively new in quantitative research on SRHR (Kapilashrami, 2020; Ritchie, 2012). Baiden et al. (2020) used the US-based Youth Risk Behavior Surveillance System (YRBSS) to investigate the intersections of race/ethnicity, sexual orientation, and suicide among 13,697 adolescents. The findings revealed that non-white sexual minority adolescents were less likely to report suicidal thoughts. When the results were adjusted for sexual orientation, the odds were 1.71 times higher among the non-white and lesbian/gay adolescents compared to their non-white and heterosexual peers (Baiden et al., 2020). Moreover, a qualitative study noted that an intersectional understanding was helpful for enabling young people with multiple marginalised positions, such as woman and bisexual, or queer and Latina, to find accessible SRHR services (Schmitz et al., 2020). Moving from the individual’s behaviour to structural prerequisites shed light on the fact that stigma and discrimination were hindering the respondents from accessing health care. These findings are also in line with a quantitative study exploring how the intersection of gender and racial/ethnic identity is associated with sexual empowerment. A sense of empowerment was found to be a determinant of sexual pleasure among non-white women but not among white men (Gusrang, 2010). Likewise, Hameed (2018) found that the intersections of gender, marital status, and urban/rural life interplayed with access to SRHR services among young people in the Maldives. This qualitative study showed that being a woman and unmarried was a vulnerable position whereas being a man and unmarried was not. In addition, the US Youth Risk Behavioral Surveillance Survey showed that sexual minorities revealed poorer health outcomes and that sexual minorities belonging to a racial/ethnic minority had even poorer health outcomes, particularly relating to substance use, sexual risk behaviours, physical/sexual violence, and suicide (Gattamorta et al., 2019). To summarise, there seems to be a growing amount of literature that shows how intersectionality can be a useful tool in order to understand vulnerability in relation to SRHR among young people. However, few studies are based on national population–based surveys which have been identified as crucial for reaching the goal of health equity (Mena et al., 2019).
Aim
The aim was to explore intersecting vulnerable positions within the three SRHR-related outcome areas: unsafe sex, sex against one’s will, and transactional sex, among young people aged 16–29, through the development of a stepwise descriptive intersecting vulnerability analysis. More specifically, the analysis explores how gender intersects with five other social determinants: sexual identity, transgender experience, perceived economy, being foreign-born, and social welfare recipiency.
Methods
Data Material
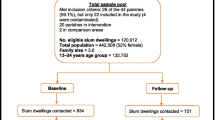
The material used is from a national stratified randomised cross-sectional survey. The survey was conducted by Statistics Sweden in 2015, in a project entitled Sexuality and Health among Young People in Sweden (The Public Health Agency of Sweden, 2017). The survey was part of the national monitoring process of the Swedish HIV prevention programme. The sampling frame was Statistics Sweden’s register of the total population of 1,730,161 individuals aged 16–29 years old on December 31st, 2014. Out of this frame, a sample of 29,997 participants was drawn. The participation of 7755 respondents gives a response rate of 26%, which was within the expected range and in line with the power estimations. A non-response analysis showed that non-participants were mainly young men, migrants, and people with low or a not completed education. To reduce the impact of the non-respondents, this information was used to create calibrated weights on the variables gender and foreign-born. The data material thus shows the likelihood of estimates for the total population, and confidence interval shows the precision (Statistics Sweden, 2015a, b).
Questionnaire
The questionnaire included 64 items, which covered several perspectives on social life in relation to SRHR. The questionnaire was piloted and validated in individual interviews with youth and young adults prior to data collection. The overall report from the pilot group was that they found the questionnaire interesting and relevant to them, and minimal changes were made. In order to avoid reducing gender to a binary male–female conceptualisation, the questionnaire also included the response option “I do not want to categorise myself”. The questionnaire also took into account whether the respondents had previously, or at the time of the survey, defined themselves as transgender. The questionnaire was responsive, and the respondents could at most be asked a total of 135 questions. However, since respondents were able to omit questions that were not relevant to them, those with no sexual onset with a partner answered a total of 43 questions.
Developing a Method for Intersectional Analysis
Research on intersectionality, which has been called a travelling theory and method, started among scholars with qualitative approaches. Ever since there has been a discussion about how to implement intersectional methods in quantitative research. The foremost debate concerns the issue of how to explore the complexity of social life in terms of social stratification since individuals belong to more than one group at the same time (Bauer et al., 2021; Hancock, 2007; Hankivsky, 2012; McCall, 2005). McCall (2005) suggested an intercategorical design that enables the analysis to start from established social categories and then use them to manage intersectionality by analysing how different groups relate to each other in a system labelled a configuration of inequality. This enables researchers to use classical statistical methods based on fundamental sociological categorisations such as gender, class, and education. Quantitative research on social life can then show the effects of the inequality layers and serve as a complement to the vast volume of qualitative research that has been conducted (McCall, 2005). Hancock (2007) suggests that data should be analysed at different levels: unitary, multiple, and intersectional, depending on how many axes of social structures a given method could handle. In the last decade, scholars have argued that this should be done using multilevel analysis and that using an additive approach needs to be avoided in favour of more complex analysis (Bauer, 2014; Bauer & Scheim, 2019; Bowleg & Bauer, 2016; Wemrell et al., 2021). This follows the idea that if each variable that predicts social life and health is first analysed separately and then added together, this will not describe more complex aspects of the phenomenon, since an intersectional analysis of power structures should be more than the sum of its parts (Collins, 2002). However, some have argued that for quantitative research, an additive approach can identify relevant effects in the context of vulnerability analyses (Reisen et al., 2013). In this paper, we locate ourselves within the latter perspective and apply a stepwise descriptive analysis resulting in a visual mapping that can be of pedagogical interest when bridging the gap between research, policy, and practice. Our analysis explores how gender intersects with the following five other social categorisations, i.e. social health determinants available in the survey data: (1) sexual identity, (2) transgender experience, (3) perceived economy, (4) being foreign-born, and (5) social welfare recipiency. These social categorisations are both structural determinants that drive vulnerability as well as identity determinants representing social groups that might be affected by the structure, i.e. society (Bauer, 2014). They also comprise groups within various fields of health research in Sweden today and correspond well with theories of intersectionality.
Measures
To test our hypothesis that intersectionality can be a useful tool in vulnerability analysis within SRHR, we used three SRHR-related outcome variables available in the survey data: unsafe sex, sex against one’s will, and transactional sex. They were chosen since they are defined as key areas for health improvement both globally and in Sweden (Guttmacher Institute, 2015; Swedish Government, 2017; The Public Health Agency of Sweden, 2020). The questionnaire item used for the analysis of unsafe sex was “Did you/your partner use any of the following types of protection or contraceptives during the most recent sexual encounter?” with the response alternative “We did not use any protection, even though it was needed”. The question captures the respondents’ experience of their most recent sexual encounter as well as all the complex aspects of how and when one should protect oneself. The questionnaire item employed in the analysis of sex against one’s will was “Have you ever experienced the following acts against your will?” with the grouped response alternatives “vaginal sexual intercourse” or “anal sexual intercourse”. The questionnaire had several more examples of sex against one’s will and was not limited to intercourse. Yet, in this analysis, we chose these two alternatives in order to give an example of intercourse without consent. The questionnaire item employed for the analysis of transactional sex was “Have you at some point received any compensation/payment for a sexual act?” with the response alternatives “yes” or “no”.
The questionnaire item employed in the analysis of gender was drawn from the register variable and included the categorisation: “Man” or “Woman”. The variable sexual identity was stated as follows in the questionnaire: “Do you consider yourself currently to be: …”, with the response alternatives: “heterosexual”, “homosexual”, “bisexual”, “I don’t usually categorise myself sexually”, “I don’t know”, or “other”. The alternatives in the analysis were limited to the first four alternatives. Those who answered “I don’t know” and “other” were removed from the analysis due to small numbers. The variable transgender experience was based on the questionnaire item “Are you or have you been a transgender person?” with the response alternatives “yes” or “no”. The variable perceived economy was based on the item “How would you describe your household finances?”, with the four response alternatives: (a) “very good”, (b) “fairly good”, (c) “not very good”, or (d) “not good at all” being grouped into two categories of alternatives a + b and c + d. The variable being foreign-born was drawn from Statistic Sweden’s register data and answers were grouped into the two categories: born in Sweden and born abroad. The variable social welfare recipiency was also based on Statistic Sweden’s register and grouped into “yes” or “no”.
Statistical Analysis
In order to analyse how gender intersects with the five other social categories or positions, sexual identity, transgender experience, perceived economy, being foreign-born, and social welfare recipiency, we developed a stepwise descriptive intersecting vulnerability analysis exemplified with the three outcome variables: unsafe sex, sex against one’s will, and transactional sex. The statistical analysis was conducted in STATA (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
The analysis was made in four steps, and the first examined prevalence in the three outcome variables based on gender only (Table 1). The second step examines gender and the five other social positions in a bivariate descriptive analysis (Table 2). The third step examines the outcome variables unsafe sex, sex against one’s will, and transactional sex based on gender and the five other intersecting social positions using cross tabulations (Tables 3, 4 and 5). The chi-square test (χ2) and Fisher’s exact test, in cells smaller than 5, were used to identify the three most vulnerable positions with significant p-values (95% CI). The fourth step involves transferring the three most vulnerable positions found in Tables 3, 4 and 5 and mapping them in a condensed scheme in order to get an overview. This final step highlights the most vulnerable positons within and between the intersections of gender and the five other social positions (Table 6). In total, the intersecting vulnerability analysis explores the indication of where the most vulnerable SRHR-related positions can be found. The analysis is built on estimations, where the confidence interval represents the uncertainties, and should be used as a way of understanding how vulnerability can be distributed in the total population.
Ethics
In Sweden, levels of general confidence in governmental agencies are relatively high. National agencies have been conducting surveys on sexuality and health since 1967 (Ministry of Education, 1969). In this context, the use of the national agency Statistics Sweden to conduct the data collection was a means of obtaining the trust of respondents. An introduction letter explained that no personal identification information would be revealed and that participants would be guaranteed that none of their information would be disclosed. The letter also contained information that the participation was voluntary and that background variables, such as sex, being born abroad (i.e. migrant), region of residence in Sweden, and receiving social welfare, would be added to each respondent’s response profile from national registers. This linking was made via the personal ID number all Swedish citizens have. After the linking, the personal ID number was replaced with an ID code specific for the survey and all tracks back to ID number were blocked in an irreversible way. This is a standard procedure for Statistics Sweden. Informed consent was held through information in the introduction letter which stated that if one submitted the questionnaire through postal service or by computer, one had also agreed to the terms of condition. As the survey included questions about sensitive topics, parents of children under the age of 18 received a separate preliminary letter explaining the research. Both the letter to the guardians and the respondents contained references to social support institutions such as the National Telephone Helpline (1177) and the online Youth Health Clinic (umo.se). The questionnaire and the study design were examined and approved by the Regional Ethical Review Board in Stockholm (ref. no.: 2015/5:4).
Results
Step 1 in the descriptive intersecting vulnerability analysis explored the prevalence in the three outcome variables of unsafe sex, sex against one’s will, and transactional sex stratified by gender. Among men, 4% reported to have had unsafe sex compared to 5% among women. Ten percent of the men reported experiences of sex against one’s will compared to 23% among women. Among men, 2% reported to have had transactional sex compared to 3% among women.
Step 2 in the descriptive intersecting vulnerability analysis explored the variations within the five social positions: sexual identity, transgender experience, perceived economy, being foreign-born, and social welfare recipiency, stratified by gender. The results showed that women (16%) reported a higher proportion of sexual minority status than men (10%). Equal shares (1%) among men and women stated that they had transgender experience, and equal shares (17%) that they had not very good or insufficient economy and equal shares (4%) had received social welfare. A slightly higher proportion of women (17%) than men (16%) were foreign-born.
Step 3 in the descriptive intersecting vulnerability analysis explored the variations within the five social positions in relation to the three SRHR-related outcome areas. The results show that the most vulnerable position for unsafe sex was being a man and homosexual (14%). The second most vulnerable position was being a woman and social welfare recipiency (11%), and the third most vulnerable position was being a man and not sufficient economy (6%) (see Table 3).
The most vulnerable position with regard to sex against one’s will was being a woman and bisexual (43%). The second most vulnerable position was being a woman and having received social welfare (40%), and the third most vulnerable position was being a woman and not sufficient economy (36%) (see Table 4).
The most vulnerable position for transactional sex was being a man and having transgender experience (26%). The second most vulnerable position for transactional sex was being a man and bisexual (12%), and the third most vulnerable position was being a woman and bisexual (9%) (see Table 5).
A Condensed Descriptive Intersecting Vulnerability Analysis
The nine most vulnerable positions identified in Tables 3, 4 and 5 are presented in Table 6. For the outcome variable unsafe sex, being a man and homosexual was the most vulnerable position. For the outcome variable sex against one’s will, being a woman and bisexual was the most vulnerable position, and for the outcome variable transactional sex, being a man and having transgender experience was the most vulnerable position. In total, the scheme presents a visual understanding of how gender intersects with the variations in the five positions and generates vulnerable positions in relation to SRHR.
Discussion
A Model for Intersecting Vulnerability Analyses
Our overall findings drawn from the stepwise descriptive intersecting vulnerability analysis show that gender intersects with the five other social positions. Even though some analytical categories are small, and the confidence intervals sometimes overlap, the findings illuminate a pattern of complexity in intersecting social determinants. Vulnerable positions within the field of SRHR were revealed, and they can be seen as sexual and reproductive health determinants that were unlocked and made visible. When investigating the overall prevalence in the three outcome variables (step 1), expected results were found: women were more vulnerable than men. However, when gender and the five other social positions were examined in a bivariate descriptive analysis (step 2), and when all positions were examined in relation to the chosen SRHR-related outcomes (step 3), we found more complex and nuanced results. Mapping the most vulnerable positions in the three outcome variables (step 4) does not solely point to women only, as a vulnerable position, but to various combinations in the intersection of gender and the five other social determinants, (a) for unsafe sex: being a man and homosexual; (b) for sex against one’s will: being a woman and bisexual; and (c) for transactional sex: being male and having transgender experience. Here it becomes clear that men can have a higher vulnerability relative to women in various SRHR-related health outcomes. The mapping presents a visual understanding of how gender intersects with other social determinants and reveals vulnerable positions in relation to SRHR. In line with Bowleg (2013), the descriptive intersecting vulnerability analysis can be used as a model for unlocking interlocked positions.
Our model of analysing and mapping intersecting vulnerable social positions in SRHR constitutes a way of clarifying the fact that gender intersects with other social determinants and that this needs to be understood in the fields of policy and practice in order to reach the most vulnerable. Using Collins (1998) definition, of how vulnerable groups tend to be marginalised and interlocked, our results first and foremost reveal that the interlocked positions in this national sample are mainly found among sexual minority youth, young people with transgender experiences, and young people having received social welfare. In line with previous research, these groups of young people might not get the same access to health services as others if they are not recognised and known (Hameed, 2018). Using an intersectional approach may also help to redirect the discussion to the issue of how we might work to include youths characterised by different social determinants, categorisations, and social positions. Being included and visible in the context of population-based SRHR surveys is vital.
Implications for Policy and Practice
The exploration of positions indicates varying vulnerability to the three SRHR-related health outcomes unsafe sex, sex against one’s will, and transactional sex. This suggests that both SRHR policy and practice need to address this complexity and tailor interventions to those who are most vulnerable. That intersectionality can be a useful way to analyse SRHR-related health outcome is in line with previous research (Bowleg, 2013; Bredström, 2008; Gusrang, 2010; Ritchie, 2012). However, our results are based on a randomised, cross-sectional national sample and provide a visual vulnerability overview. The findings may therefore contribute to the development of more tailored national surveys that can inform policy and practice. Our findings suggest that policymakers should develop national data that adopt a more inclusive approach to categories such as sexual minorities, people with transgender experience, and social welfare recipients. In summary, there is a need to move forward and use an intersectional perspective in quantitative research on SRHR in a way that can inform policy and thus guide practice. In line with previous research (Kapilashrami, 2020; Ritchie, 2012), our results support the idea that if the vision of health equity is to be realised, along with the inclusive perspective of the UN Agenda 2030 to leave no one behind, there is a need for policies and programmes to reflect the diversity and complex aspects of social life and SRHR.
Methodological Strengths and Limitations
Since social life is in constant change, therefore we need to be cautious about the time and context of our findings. Vulnerable positions may differ between different societies and may shift within the same society. This means that the vulnerable positions identified in this study are relevant to the Swedish context, or to similar countries. At the same time, the method of using an intersecting vulnerability analysis can be applicable to a wide range of contexts and countries.
As a result of Statistics Sweden’s access to register data on age, gender, place of birth, economy, and education in the total population, our statistical analysis has had valuable sociodemographic information about both the respondents and non-respondents, which has added to the validity and reliability of the findings. The study design allowed for corrections for the non-respondents’ gender and place of birth; these adjustments have been weighted into the responses that had already been given. Despite this design, there is still a risk that some demographic groups have higher representation than others. It is therefore possible that our results may tend, in some respects, to describe young people who have relatively good socioeconomic conditions. Another limitation is that the questionnaire did not have variables focusing on ethnicity and disability. Studies that include these perspectives are needed. In this paper, we did not explore education as a possible social determinant for vulnerability to SRHR. This has to do with the fact that Swedish young people finalise their higher education quite late in life compared to other European countries (OECD, 2021; The Swedish Government, 2011). However, for future research, it can be of interest to include this perspective.
In 2015, a large number of young immigrants arrived in Sweden as unaccompanied minors, most of whom were young men from Asia. It should be noted that this group was not included in this study. For this reason, the figures presented for migrants will be interesting to follow in future surveys. With this in mind, there is always a need for national population–based surveys to be complemented with data collection in groups that share socio-demographic characteristics with the non-respondents.
In order to carry out the analyses with as much inclusion as possible, it was our intention to include both transgender and non-binary gendered people. However, unfortunately, a cross tabulation and analysis of too many small groups would not have produced trustworthy results which made us leave non-binary gender outside our analysis and use the register variable sex. On the other hand, the questionnaire items made it possible to include some of the smaller groups like transgender people, who are often overlooked in statistical analysis. Even though the analytical categories sometimes are small, and the confidence intervals overlap, it is still valuable to include these groups to learn more about indications of estimates and health outcomes in a population. We acknowledge Mahendran et al. (2022) when they state that using intersectionality in quantitative research is not only a methodological choice, it also involves illuminating power relations that create vulnerabilities and marginalisation. Also, we do believe that a visible scheme, the mapping of the most vulnerable positions, can be a pedagogical way to show the need for using intersectionality in SRHR research.
The three outcome variables can at first sight seem to mainly be associated with sexual health and not with reproductive health. Yet, there is an overlap between these areas, as reproductive health also needs to be founded in sexual health and human rights associated to both areas (Starrs et al., 2018; The Public Health Agency of Sweden, 2020). There are also findings showing that bisexual women have a higher proportion of abortion than their heterosexual peers (Charlton et al., 2020). In light of this, the intersection of sexual identity and unsafe sex is an area of reproductive health. To include these aspects is also a way of including bisexual women which is a group that has often been overlooked in research on reproductive health (Moegelin et al., 2010). Also, lack of mental and social well-being among young people in Sweden involved in transactional sex (Fredlund et al., 2018; RFSL, 2011) may have implications on both sexual and reproductive health with regard to the definition in the Guttmacher-Lancet report (Starrs et al., 2018).
Conclusions
There is a need for policies and population-based surveys to be complemented with an intersectional understanding of vulnerable positions in relation to SRHR. The stepwise descriptive intersecting vulnerability analysis presents a visual understanding and indicates how gender intersects with sexual identity, transgender experience, perceived economy, being foreign-born, and social welfare recipiency, and creates vulnerable positions. Although based on a national sample, the analysis can be of global interest and value. The use of an intersectional approach, in SRHR policy and thus in future population-based survey analyses, can move the field further towards the transformative goal of a sustainably society in line with the UN Agenda 2030 in which no one is left behind.
References
Andersson, G. (2019). Quality of life and sexual health among transgender people and people living with HIV in Sweden. AIDS Care, 31(4), 403–412.
Baiden, P., LaBrenz, C., Asiedua-Baiden, G., & Muehlenkamp, J. J. (2020). Examining the intersection of race/ethnicity and sexual orientation on suicidal ideation and suicide attempt among adolescents: Findings from the 2017 Youth Risk Behavior Survey. Journal of Psychiatric Research, 125(13–20).
Bauer, G. R. (2014). Incorporating intersectionality theory into population health research methodology: Challenges and the potential to advance health equity. Social Science & Medicine, 110, 10–17.
Bauer, G. R., Churchill, S. M., Mahendran, M., Walwyn, C., Lizotte, D., & Villa-Rueda, A. A. (2021). Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods. SSM-Population Health, 14, 100798.
Bauer, G. R., & Scheim, A. I. (2019). Advancing quantitative intersectionality research methods: Intracategorical and intercategorical approaches to shared and differential constructs. Social Science & Medicine, 226, 260–262.
Berkman, L., Kawachi, I., & Glymour, M. M. (2014). Social epidemiology. Oxford University Press.
Bowleg, L. (2008). When Black + lesbian + woman ≠ Black lesbian woman: The methodological challenges of qualitative and quantitative intersectionality research. Sex Roles, 59(5–6), 312–325.
Bowleg, L. (2012). The problem with the phrase women and minorities: Intersectionality—An important theoretical framework for public health. American Journal of Public Health, 102(7), 1267–1273.
Bowleg, L. (2013). Once you’ve blended the cake, you can’t take the parts back to the main ingredients: Black gay and bisexual men’s descriptions and experiences of intersectionality. Sex Roles, 68, 754–767.
Bowleg, L., & Bauer, G. (2016). Invited reflection: Quantifying intersectionality. Psychology of Women Quarterly, 40, 337–341.
Bredström, A. (2008). Safe sex, unsafe identities: Intersections of ‘race’, gender and sexuality in Swedish HIV/AIDS policy. Linköping University.
Charlton, B. M., Everett, B. G., Light, A., Jones, R. K., Janiak, E., Gaskins, A. J., Chavarro, J. E., Moseson, H., Sarda, V., & Austin, S. B. (2020). Sexual orientation differences in pregnancy and abortion across the lifecourse. Women’s Health Issues, 30(2), 65–72.
Collins, P. H. (1998). It’s all in the family: Intersections of gender, race, and nation. Hypatia, 13(3), 62–82.
Collins, P. H. (2002). Black feminist thought: Knowledge, consciousness, and the politics of empowerment. Routledge.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of colour. Stanford Law Review, 43(6), 1241–1299.
Fredlund, C., Dahlström, Ö., Svedin, C. G., Wadsby, M., Jonsson, L. S., & Priebe, G. (2018). Adolescents’ motives for selling sex in a welfare state – A Swedish national study. Child Abuse & Neglect, 81, 286–295. https://doi.org/10.1016/j.chiabu.2018.04.030
Gahagan, J., & Bryson, M. K. (2021). Sex- and gender-based analysis in public health. Geneva: Switzerland Springer Nature. http://link.library.eui.eu/portal/Sex--and-Gender-Based-Analysis-in-Public-Health/uNVHYyhugaI/
Gattamorta, K. A., Salerno, J. P., & Castro, A. J. (2019). Intersectionality and health behaviors among US high school students: Examining race/ethnicity, sexual identity, and sex. Journal of School Health, 89(10), 800–808. https://doi.org/10.1111/josh.12817
Gusrang, J. L. (2010). Removing the “risk” from adolescent sexual behavior: An intersectional analysis of adolescent sexual empowerment. Doctoral dissertation, University of Connecticut.
Guttmacher Institute. (2015). Sexual and reproductive health and rights indicators for the SDGs. Recommendations for inclusion in the Sustainable Development Goals and the post-2015 development process. [Internet]. https://www.guttmacher.org/sites/default/files/report_pdf/srhr-indicators-post-2015-recommendations.pdf
Hameed, S. (2018). To be young, unmarried, rural, and female: Intersections of sexual and reproductive health and rights in the Maldives. Reproductive Health Matters, 26(54), 61–71. https://doi.org/10.1080/09688080.2018.1542910
Hammarstrom, S., Tikkanen, R., & Stenqvist, K. (2015). Identification and risk assessment of Swedish youth at risk of chlamydia. Scandinavian Journal of Public Health, 43(4), 399–407. http://www.ncbi.nlm.nih.gov/pubmed/25740618
Hancock, A.-M. (2007). When multiplication doesn’t equal quick addition: Examining intersectionality as a research paradigm. Perspectives on Politics, 5(1), 63–79.
Hankivsky, O. (2012). Women’s health, men’s health, and gender and health: Implications of intersectionality. Social Science & Medicine, 74(11), 1712–1720. http://www.ncbi.nlm.nih.gov/pubmed/22361090
Johansson, K., Persson, K. I., Deogan, C., & El-Khatib, Z. (2018). Factors associated with condom use and HIV testing among young men who have sex with men: A cross-sectional survey in a random online sample in Sweden. Sexually Transmitted Infections, 94(6), 427–433.
Kapilashrami, A. (2020). What is intersectionality and what promise does it hold for advancing a rights-based sexual and reproductive health agenda? BMJ Sexual & Reproductive Health, 46(1), 4–7.
Mahendran, M., Lizotte, D., & Bauer, G. R. (2022). Quantitative methods for descriptive intersectional analysis with binary health outcomes. SSM-Population Health, 101032.
Marmot, M. (2005). Social determinants of health inequalities. The Lancet, 365(9464), 1099–1104.
Marmot, M., & Wilkinson, R. (2005). Social determinants, sexual behaviour, and sexual health. Social Determinants of Health. Oxford: Oxford University Press. http://www.oxfordscholarship.com/view/10.1093/acprof:oso/9780198565895.001.0001/acprof-9780198565895-chapter-15
McCall, L. (2005). The complexity of intersectionality. Signs: Journal of Women in Culture and Society, 30(3), 1771–1800. https://doi.org/10.1086/426800
Mena, E., Bolte, G., Bolte, G., Mena, E., Rommel, A., Saß, A.-C., Pöge, K., Strasser, S., Holmberg, C., Merz, S., Jaehn, P., & on behalf of the, A. G. S. G. (2019). Intersectionality-based quantitative health research and sex/gender sensitivity: A scoping review. International Journal for Equity in Health, 18(1), 199. https://doi.org/10.1186/s12939-019-1098-8
Ministry of Education. (1969). About sexual life in Sweden. Values, norms and behaviors in sociological interpretation. Stockholm, Sweden. https://docplayer.se/223213354-Om-sexuallivet-i-sverige.html
Moegelin, L., Nilsson, B., & Helström, L. (2010). Reproductive health in lesbian and bisexual women in Sweden. Acta Obstetricia Et Gynecologica Scandinavica, 89(2), 205–209. https://doi.org/10.3109/00016340903490263
OECD. (2021). Education at a Glance 2021 - OECD Indicators. Paris. https://www.oecdilibrary.org/education/education-at-a-glance-2021_b35a14e5-en
Persson, K. I. (2018). Relating to risk: Sexual behaviour and risk perception among men who have sex with men. Department of Public Health Sciences. Stockholm, Karolinska Institutet. https://openarchive.ki.se/xmlui/handle/10616/46352
Persson, K. I., Berglund, T., Bergström, J., Eriksson, L. E., Tikkanen, R., Thorson, A., & Forsberg, B. C. (2016). Motivators and barriers for HIV testing among men who have sex with men in Sweden. Journal of Clinical Nursing, 25(23–24), 3605–3618.
Reisen, C. A., Brooks, K. D., Zea, M. C., Poppen, P. J., & Bianchi, F. T. (2013). Can additive measures add to an intersectional understanding? Experiences of gay and ethnic discrimination among HIV-positive Latino gay men. Cultural Diversity and Ethnic Minority Psychology, 19(2), 208.
RFSL. (2011). Osynliga synliga aktörer. HBT-personer med erfarenhet av att sälja och/eller köpa sexuella tjänster. Stockholm, Riksförbundet för homosexuellas bisexuellas transpersoners och queeras rättigheter (RFSL). https://www.rfsl.se/wp-content/uploads/2019/01/RFSL_Osynliga_Synliga_Akto%CC%88rer.pdf
Ritchie, A. (2012). Intersectionality and the struggle for sexual and reproductive health and rights: An analysis of UN discursive patterns. Victoria, New Zealand: University of Wellington. http://researcharchive.vuw.ac.nz/handle/10063/2270
Schindele, A. C., & Lindroth, M. (2020). Sexual and reproductive health and rights (SRHR) among young people in secure state care and their non-incarcerated peers–A qualitative, descriptive and comparative study. European Journal of Social Work, 1–14.
Schmitz, R. M., Robinson, B. A., & Tabler, J. (2020). Navigating risk discourses: Sexual and reproductive health and care among LBQ+ Latina young adults. Sexuality Research and Social Policy, 17(1), 61–74.
Starrs, A. M., Ezeh, A. C., Barker, G., Basu, A., Bertrand, J. T., Blum, R., Coll-Seck, A. M., Grover, A., Laski, L., & Roa, M. (2018). Accelerate progress—Sexual and reproductive health and rights for all: Report of the Guttmacher–Lancet Commission. The Lancet.
Statistics Sweden. (2015a). Cognitive interviews of adolescents' sexual health [Kognitiva intervjuer ungas sexuella hälsa. Enheten för mätteknik. Prod.nr 8762668. för Folkhälsomyndigheten. DIH/ENK, SCB]. Örebro.
Statistics Sweden. (2015b). Technical report. A description of implementation and methods - Adolescents' sexual health (UngKAB15) [Teknisk Rapport. En beskrivning av genomförande och metoder - Ungas sexuella hälsa (UngKAB15)]. Örebro.
Swedish Government. (2017). National strategy on HIV and other infectious diseases. Stockholm. https://www.regeringen.se/informationsmaterial/2017/12/nationell-strategi-mot-hivaids-och-andra-smittsamma-sjukdomar/
The Public Health Agency of Sweden. (2017). Sexuality and health among young people in Sweden. UngKAB15 – A survey on knowledge, attitudes and behaviour among young people 16–29 years old. Sweden: The Public Health Agency of Sweden. https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/s/sexuality-and-health-among-young-people-in-sweden/
The Public Health Agency of Sweden. (2020). National strategy for sexual and reproductive health and rights (SRHR) in Sweden. Solna, Sweden. https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/n/nationell-strategi-for-sexuell-och-reproduktiv-halsa-och-rattigheter-srhr/
The Swedish Government. (2011). Långtidsutredningen 2011 (The long-term investigation in the labour market). Stockholm. https://www.regeringen.se/49bb35/contentassets/2969767dc25446d69a200f2d1b579744/sou-201111-langtidsutredningen-2011-huvudbetankande
UN. (1995). Beijing Declaration and Platform for Action (PoA). Beijing, China: The United Nations, United Nations Population Fund. https://www.un.org/womenwatch/daw/beijing/pdf/BDPfA%20E.pdf
UN. (2013). General comment No. 15 (2013) on the right of the child to the enjoyment of the highest attainable standard of health (art. 24). Geneva, The United Nations, The Committee on the Rights of the Child. http://docstore.ohchr.org/SelfServices/FilesHandler.ashx?enc=6QkG1d%2FPPRiCAqhKb7yhsqIkirKQZLK2M58RF%2F5F0vHCIs1B9k1r3x0aA7FYrehlNUfw4dHmlOxmFtmhaiMOkH80ywS3uq6Q3bqZ3A3yQ0%2B4u6214CSatnrBlZT8nZmj
UN. (2015). Transforming our world - The 2030 Agenda for sustainable development. New York, The United Nation, General Assembly. https://sustainabledevelopment.un.org/post2015/transformingourworld/publication
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., & Currie, C. (2012). Adolescence and the social determinants of health. The Lancet, 379(9826), 1641–1652.
Wemrell, M., Karlsson, N., Vicente, R. P., & Merlo, J. (2021). An intersectional analysis providing more precise information on inequities in self-rated health. International Journal for Equity in Health, 20(1), 1–10.
WHO. (2016). Action plan for sexual and reproductive health. Towards achieving the 2030 Agenda for Sustainable Development in Europe – leaving no one behind. Denmark. https://www.euro.who.int/__data/assets/pdf_file/0003/322275/Action-plan-sexual-reproductive-health.pdf
Wolitski, R. J., & Fenton, K. A. (2011). Sexual health, HIV, and sexually transmitted infections among gay, bisexual, and other men who have sex with men in the United States. AIDS and Behavior, 15(1), 9–17.
Acknowledgements
The authors would like to thank Lars Plantin and Anna Bredström for valuable input on an earlier draft of the paper, and Henrik Källberg for valuable input on the statistical analysis.
Funding
Open access funding provided by Malmö University. This work was supported by the Public Health Agency of Sweden. The funder had no influence on the process or conclusions of the present work. The views expressed are those of the authors and not necessarily those of the funder.
Author information
Authors and Affiliations
Contributions
Conceptualization: Anna ChuChu Schindele; methodology: Anna ChuChu Schindele; formal analysis and investigation: Anna ChuChu Schindele; writing—original draft preparation: Anna ChuChu Schindele; writing—review and editing: Anna ChuChu Schindele, Kristina Areskoug Josefsson, Malin Lindroth; funding acquisition: Anna ChuChu Schindele; supervision: Malin Lindroth and Kristina Areskoug Josefsson.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Informed consent has been achieved as all study participants have been given the opportunity to receive written information about the study and the opportunity to refrain from participating. This study was examined and approved by the Regional Ethical Review Board in Stockholm (ref. no.: 2015/5:4).
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schindele, A.C., Areskoug Josefsson, K. & Lindroth, M. Vulnerability Analysis in Sexual and Reproductive Health and Rights (SRHR) — Indications of Intersecting Vulnerable Positions in a National Survey Among Young People in Sweden. Sex Res Soc Policy 19, 1034–1045 (2022). https://doi.org/10.1007/s13178-022-00742-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13178-022-00742-7